DEFINITION — A myocardial infarction, or MI, is commonly known as a heart attack. An MI is damage to an area of the heart muscle that is caused by a lack of blood supply.
Not every MI is the same. Treatment decisions will be made, in part, based upon the type and severity of MI experienced by the patient.
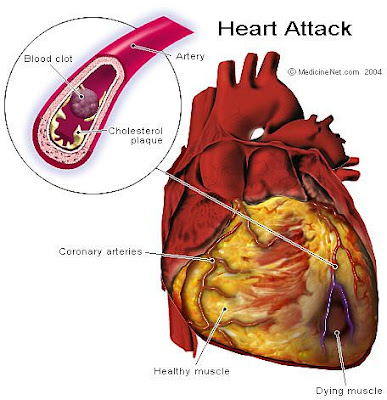
CAUSES — Almost all cases of MI occur in someone who has an underlying condition called coronary heart disease (CHD), which is due to narrowings or blockages in the coronary arteries, known as plaques. MI occurs when the plaque ruptures and causes a blood clot (thrombus) to form in one of the coronary arteries. CHD and blood clot formation in MI are explained in turn below.
Coronary heart disease — All the organs and tissues in the body need a blood supply in order to function normally; blood carries oxygen and energy sources, especially sugar or glucose, that are required to meet the body's needs. It is the heart's job to pump oxygen-rich blood through the huge network of arteries that extend throughout the body, and this includes pumping blood into the vessels that supply the heart muscle itself. These vessels, called coronary arteries, lie on the outside of the heart muscle before entering the heart muscle itself (show figure 1).
In coronary heart disease (CHD), the coronary arteries become clogged with fatty deposits. The deposits, called plaques, cause a narrowing of the arteries through which the blood reaches the heart muscle (show figure 2). This can create an imbalance between the supply of blood (or oxygen) available to an area of heart muscle and the demand for blood (or oxygen) that is needed at a given moment. This causes a condition known as ischemia, sometimes felt by the patient as chest discomfort (angina pectoris).
Plaque rupture and clot formation — Sometimes a plaque in a coronary artery bursts or ruptures, leading to the formation of a blood clot that may partially or completely block the artery. A blockage of this type is likely to cause damage to the heart muscle due to a lack of blood and oxygen supply. If there is damage, an MI, or heart attack, has occurred.
The factors leading to the rupture of a plaque and the formation of a blood clot are not completely understood. There are certain characteristics related to the composition of a plaque that seem to make it vulnerable to rupture. Plaques that have an irregular appearance may contain less calcium and scar tissue and more lipids (fat) within their core, and may be more prone to rupture. Intense physical activity or psychologic stress immediately preceding MI may play a role because these activities affect the heart rate and blood pressure and could cause disruption of a plaque.
Some studies have shown that an emotional or stressful event occurs in a certain percentage of people in the days or hours before an MI. In addition, an increase in the incidence of MI has been noted in populations where a disaster has occurred. Because mental stress is known to cause increases in heart rate and blood pressure as well as other changes in the cardiovascular system, it has been suggested that, in some cases, mental stress can affect the stability of a coronary artery plaque and "trigger" an MI.
SYMPTOMS — The "typical" complaint of a person having an MI is persistent chest discomfort, resulting from ischemia involving an area of heart muscle. But there is wide variability in the symptoms a person can have when an MI is occurring. Some patients have no symptoms at all. Others, particularly women, older adults, diabetics, and individuals with a prior diagnosis of heart failure, may have other symptoms but not report chest discomfort. Still others have a combination of chest discomfort and other complaints. Some people having an MI will experience sudden death, also known as cardiac arrest.
Ischemic chest pain in angina and MI — Recall that the obstruction in blood flow that occurs in patients with CHD can cause an imbalance between the supply of oxygen-rich blood to an area of heart muscle and the demand for oxygen that exists at a point in time. This causes a relative lack of oxygen to the muscle, or ischemia, and may be felt by the patient as chest discomfort or angina pectoris. When the imbalance is eventually corrected during the anginal episode—for example, the person may rest, thereby decreasing the heart's oxygen demand—the discomfort slowly goes away and no damage has occurred.
The chest discomfort that occurs in the setting of an MI, caused by a blood clot that more seriously obstructs blood flow, can be similar to an episode of angina, because it also arises from ischemia to the heart. It may last longer (an episode of angina usually lasts more than two but less than 20 minutes), and may not be relieved by the measures that often relieve angina, such as rest or the use of nitroglycerin under the tongue.
Many different conditions can cause pain in the chest. The ischemic chest discomfort of an MI can range from mild to severe, and typically has the following characteristics:
* Felt as a pressure, constriction, tightness, or squeezing, versus a sharp or stabbing pain
* Is not limited to a small area, but rather spreads through the chest
* May radiate to other areas of the body, including the upper abdomen, shoulders, arms, neck and throat, or lower jaw and teeth
* Comes on gradually and lasts more than a few seconds
* Is usually not made worse by pressing on the area of the chest that is affected, by taking a deep breath or by a particular position; however, lying down may make it worse, while sitting up may produce some reduction in intensity
* Is not relieved by antacids or food
Other symptoms of MI — A number of other symptoms can occur in the setting of an MI. They may occur in a patient with or without chest discomfort. These include:
* Shortness of breath
* Nausea, vomiting, or belching
* Sweating
* Palpitations
* Lightheadedness
* Fatigue
* Fainting
* Cardiac arrest (sudden cardiac death)
DIAGNOSIS — The doctor uses a combination of tools to diagnose MI. The main tools are:
History and physical exam — The healthcare provider will gather information about any symptoms the patient may have experienced and analyze the person's risk of having CHD. Chest discomfort in someone with multiple risk factors for CHD raises the suspicion that the discomfort is cardiac in origin. (See "Patient information: Chest pain"). A complete physical exam may reveal signs of ischemia, such as abnormal heart sounds or cardiac rhythm.
Electrocardiogram — An electrocardiogram, or ECG, gives a picture of the flow of electrical activity that causes the heart to beat. Damaged or ischemic areas may (or may not) show an abnormal pattern. There are very specific patterns that are associated with an MI, and the ECG is usually the most important method for diagnosing an acute MI.
Blood tests — In the hours following a suspected MI, the blood can be monitored for substances (enzymes or proteins) released by damaged heart muscle. The presence of these substances in certain concentrations suggests that heart damage, or MI, has occurred.
TYPES OF MI — There are different types of MI, based partly on the area of the heart that is damaged and partly on the extent of damage as visualized on the ECG.
Location — Depending on which coronary arteries are obstructed, different areas of the heart can suffer damage during an MI. The areas most frequently affected include:
* Anterior MI
* Inferior MI
* Lateral MI
* Posterior MI
* Right ventricular MI
ST elevation MI (STEMI) versus non-ST elevation MI (NSTEMI) — The wave patterns on an ECG provide information about how the heart is functioning (show figure 3). In general, an ST elevation MI is caused by complete obstruction of a coronary artery, and causes damage that involves the full thickness of the heart muscle. In contrast, a non-ST elevation MI is caused by partial obstruction of a coronary artery, and causes damage that does not involve the full thickness of the heart wall. The treatment for these two types of MIs may differ.
TREATMENT — Acute MI refers to a heart attack that is in progress, as opposed to one that has occurred at some time in the past. Treatment decisions are based in part on whether the patient has had a STEMI or NSTEMI. Other factors, such as the patient's age, extent of CHD, and complications that have occurred also help direct treatment. A full discussion of treatments given during and immediately after is available separately. (See "Patient information: Heart attack treatment"). Recovery after heart attack is also discussed separately. (See "Patient information: Heart attack recovery").
COMPLICATIONS — Treatment of acute MI is more effective than in years past, and patients in general have a better expectation of a favorable outcome. Still, complications can occur, and include:
Ongoing ischemia — Early treatments may fail to halt the ischemic process and expanding areas of the heart may become damaged.
Abnormal heart rhythms — The damaged heart muscle can cause disturbances in the way the electrical impulses, which activate the muscle and cause the heart to beat, travel within the heart. An erratic heart beat and/or abnormal heart rhythm can result, some of which can lead to poor heart function or sudden cardiac death.
Poorly functioning left ventricle — If the heart's main pumping chamber, the left ventricle, is seriously damaged, its ability to function can be impaired. This can lead to a number of related complications (show figure 4).
* Heart failure — Heart failure refers to a condition in which the ventricle is stiff or weak, meaning that it has difficulty pumping blood in the normal way.
* Low blood pressure — Low blood pressure can occur, risking lack of adequate blood flow to the rest of the body, especially the brain.
* Cardiogenic shock — Cardiogenic shock can develop if the weakness of the heart is very severe and the amount of blood it pumps out very reduced; as a result, all the organs and tissues of the body suffer from lack of blood flow.
Left ventricular aneurysm — This refers to an area of left ventricle that has become thin and scarred and bulges outward, moving ineffectively during contraction. Left ventricular aneurysm can lead to a poorly functioning left ventricle, described above. If the wall is very thinned, the aneurysm may rupture, usually resulting in death.
Mechanical problems — An MI can cause the rupture of the muscles that hold the mitral valve in place; this valve, located between the left atrium and left ventricle, prevents blood from flowing back into the left atrium when the left ventricle contracts (show figure 4). If the valve is damaged, or insufficient, there is an abnormal flow between these two chambers, known as mitral regurgitation. Rupture of the membrane separating the left and right heart chambers can also occur, as can rupture of the wall of the ventricle.
These complications can be treated to a greater or lesser degree of success, depending upon a wide variety of factors, including early diagnosis, seriousness of the complication, and availability of appropriate interventions (for example, PTCA or cardiac surgery).
PREVENTION — Although MI cannot always be prevented, there are a number of good health practices that can reduce the chance that a person will have an MI.
Quitting smoking, controlling blood pressure and diabetes, and reducing blood cholesterol levels reduce a person's overall risk for developing CHD and MI. (See "Patient information: Smoking cessation" and see "Patient information: High blood pressure treatment in adults" and see "Patient information: High cholesterol and lipids (hyperlipidemia)").
In some patients, taking a low dose of aspirin every day is recommended as a way to reduce the risk of heart attack and stroke, but this should not be done without consulting with a healthcare provider. (See "Patient information: Aspirin and cardiovascular disease").
Finally, good routine medical care (going to the doctor for regular check-ups) may mean that early signs of CHD are detected when steps can be taken that may prevent a future MI.


